


Keratoconus is a bilateral, asymmetric corneal ectasia and typically affects patients in their second or third decade of life.1,2 Clinicians often spend significant chair time and patient education efforts counseling patients who have keratoconus regarding their condition. Diagnosing keratoconus proves challenging, as healthcare providers often detect it during a phase of life when other systemic medical diagnoses are non-existent or few.
Due to recent advances in corneal imaging technology, increased awareness among practitioners, and the availability of corneal cross-linking (CXL) to prevent progression, we are now able to diagnose and treat young patients who have keratoconus sooner than ever; indeed, recent prevalence data suggest we must place greater emphasis on early screening and diagnosis.3,4
Recognizing the signs of corneal ectasia during a careful slit lamp examination (apical thinning, Vogt striae, Fleisher ring, central scarring) can help with early diagnosis—and increase the impact of early intervention with corneal collagen cross-linking. Doing so can help with prevention of vision loss, and may decrease the emotional impact and functional deficits that can follow.5-9 Specialty contact lenses can play a key role in managing corneal ectasia, with or without vision loss.10-12
Corneal Imaging
Corneal imaging plays a key role in the early diagnosis of keratoconus and in our annual assessment to monitor progression. While corneal tomography provides the most comprehensive evaluation, corneal topography can and should still be utilized when tomography is not available. However, topography has limitations, as it cannot assess the posterior corneal surface or provide detailed information regarding global corneal thickness and enhanced ectasia screening.13
When using corneal topography and tomography for making the diagnosis of keratoconus, start with the refractive maps and implement a systematic assessment of the result:
Axial maps: When assessing an axial map, assess whether the astigmatic “bow-tie” pattern is asymmetric, skewed (often described as an asymmetric “bow-tie” appearance), or bent. A manuscript by Matilia and Swarup presents sketches of normal and various keratoconic axial maps.14 Consider a pattern skewed between 12° to 15° as suspicious, while those skewed >30° are likely abnormal.
Elevation maps: When assessing the elevation maps, envision you are dividing them in half, from side to side, and then from top to bottom. Assess whether they look similar on either side of your dividing lines. Asymmetry can be suspicious, as can tomography that shows increased elevation at the thinnest point of the cornea.
Pachymetry maps (tomography): Determine whether the thinnest point/minimum pachymetry reading is within 1.0 mm of the “vertex normal” (or line of sight). Assess the isopachs going from inside to out—are they round (normal) or oval (more suspicious)? Assess for asymmetry in the minimum pachymetry reading between the eyes. The normal expected difference is 5µm to 6µm. When the difference is >17 µm, this is considered abnormal.
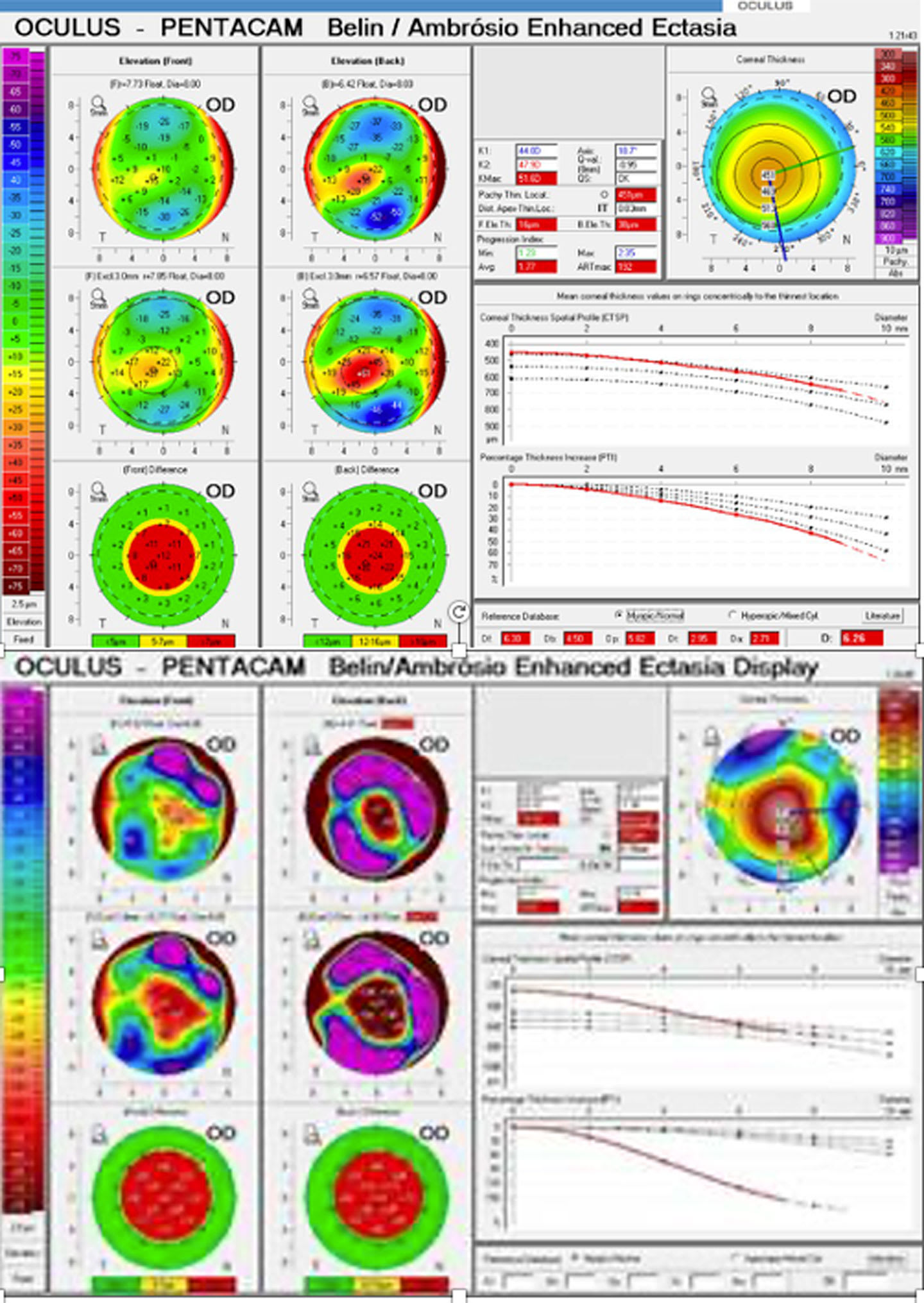
Ectasia maps (tomography): Look for irregularities in the difference maps, corneal thickness, and percentage thickness increase (above or below the 2 standard deviations). Consider a final Belin/Ambrosio Enhanced Ectasia Display (BAD-D) value of >1.6 as suspicious, >2.0 suspect, and >2.6 definitive (though some studies use >3.0 as a more conservative cutoff score for diagnosis).3,4,15
Another common clinical question is how often to re-evaluate patients when the diagnosis is uncertain, following imaging and analysis using the above methods. Table 1 presents a follow-up timeline for repeat imaging based upon patient age. Ensure the ocular surface is appropriately managed and that any dry eye is mitigated before, during, and after this imaging and diagnosis phase, as corneal staining can affect front-surface imaging results, and dry eye can prevent contact lens success.16,17
Table 1: Recommended follow-up intervals if no definitive diagnosis
|
Patient age |
Follow-up |
|
<20 years old |
4-6 weeks |
|
20-30 years old |
3 months |
|
30-40 years old |
6 months |
|
>40 years old |
Annually |
For examinations without access to tomography, topographic metrics can be used to assess for ectasia. Adding ultrasonic pachymetry in a few inferior areas of the cornea (correlate these points with the steepest areas on the tangential topography map prior) can help to confirm whether thinning is present. Anterior segment optical coherence tomography (AS-OCT) imaging can also assess corneal thickness of cross-sectional images using software caliper tools and (if available) epithelial thickness metrics to further confirm the diagnosis. AS-OCT imaging can also be useful for fitting/evaluating scleral lenses in these patients.18
Patient Education
Patient education should start with explaining corneal ectasia; the risk of progression (including prevention by not rubbing the eyes); the management of any associated systemic disease, allergy, or atopic conditions; the risk of development of corneal hydrops (including the potential symptoms of hydrops); and the availability of CXL to prevent progression. Contact lens options should be discussed (see recommendations below) and fit when the patient is ready, following release from CXL post-operative visits if that procedure is imminent. Be sure to recommend that family members, including any children or siblings, undergo screening for corneal ectasia.
With regard to eye rubbing, keratoconus patients tend to rub their eyes with their palm, fist, or knuckles, causing histamine release and subsequent corneal effects.19-23 It can be helpful to ask the patient to “show me how you rub your eyes,” as they may not be consciously aware of what they are doing and can work to stop this habit once it is recognized.
Patients who have keratoconus may also experience effects on their quality of life and mental health. The Collaborative Longitudinal Evaluation of Keratoconus (CLEK) study was the first to report a similar correlation, surveying patients on quality of life and determining that despite having a mean entrance best-corrected visual acuity (BCVA) of 20/15, patients who have keratoconus report quality of life scores similar to patients with Category 4 AMD (advanced with significantly reduced VA).
Another review of 31 studies on the topic of keratoconus and mental health found that keratoconus patients have mental health scores disproportionate to the effect on visual acuity.8 Patients who have keratoconus seem to also have worse mental health outcomes when they have reduced BCVA (in either their better or worse eye) and/or significant asymmetry between the eyes.24 Thus, even in patients who have keratoconus as well as relatively good visual acuity, mental health can suffer.
In studies commenting on mental health outcomes by examining the “emotional domains” of quality of life, most found a correlation between keratoconus severity and worsening emotional state.25 Very often, these quality-of-life issues revolve around frustration, fear, cost, and feelings of isolation and discrimination, and they persist regardless of intervention/treatment.9
Given the progressive nature of keratoconus, patients managing with spectacles and contact lenses may note a significant decline in BCVA and, subsequently, in functional visual acuity, which can affect overall well-being.17 Asking patients how they are feeling about their eyes may be a helpful way to allow patients to ask questions about their fears and future concerns and allay some worries during an examination. Continuing to provide education and resources for patients who need them can be a helpful way to support “the whole person” while also caring for a patient’s eyes.
Contact Lens Selection
A wide range of contact lens options exist for patients who have keratoconus (Table 2); however, attention should be paid to the severity of the disease, the individual patient’s needs, and prior lens-wearing experience (including failure with prior designs) before selecting. Lens options range from simple to complex, and a patient-centered discussion is warranted prior to beginning the fitting process, which will include expectations on the length of the process, expectations for follow-up, costs involved, and management strategies. Clinical data needed to make an assessment include case history, visual acuity (via manifest refraction and, if necessary, a corneal GP lens over-refraction), and topography or tomography.
Table 2: Contact lens options for patients who have keratoconus
| Soft contact lenses |
| Specialty soft contact lenses |
| Corneal gas permeable lenses |
| Piggyback systems |
| Hybrid len |
For soft contact lenses, practitioners can consider spherical, toric, and extended-range toric designs. To fit these designs successfully, the lens must be stable, adequately drape the cornea, avoid inferior lift-off, and provide adequate vision correction. Specialty soft contact lenses often incorporate aspheric toric optics and have a larger center thickness (0.2 mm to 0.4 mm) to correct irregular astigmatism. However, if best-corrected spectacle acuity is worse than 20/40, specialty soft lenses may not correct enough irregular astigmatism to achieve visual success.
Corneal GP lenses are a mainstay of vision correction and can range from tricurve and pentacurve designs fit with 3-point-touch to keratoconic and limbal designs with aspheric peripheral curves, variable optic zones, and inferior steepening options catered toward the typical corneal shape seen in keratoconus. Corneal lenses can also be used over a soft lens carrier as a piggyback system to prevent corneal staining, improve lens centration, or improve comfort if needed. Concerns with a piggyback system can include handling challenges, risk of reduced oxygen transmission, and the need for more than 1 disinfection system or case.
Hybrid lenses can relieve some of these handling challenges by providing a GP lens center bonded to the soft lens skirt. Keratoconus-specific hybrid lens designs can provide sufficient prolate geometry in the GP center to accommodate mild-moderate cones; however, the vault may be limited, or ultimately insufficient, in very advanced ectasia. Those very diseased prolate eyes may require the flexibility and customization that comes with a scleral lens design.
Scleral lenses can be fit in a straightforward manner using a diagnostic fitting set, and quadrant-specific adjustments to various aspects of the lens (corneal chamber, limbal/transition zone vault, and edge landing) can be requested, along with edge vaults/recesses/notches, as indicated and available from the manufacturer. If indicated, front-surface toric optics, front-surface eccentricity, or wavefront-guided, higher-order aberration correction are available.
In the most complex of cases using profilometry-guided scleral lens fitting methods or impression-molded scleral lens options may be indicated. One study found that scleral lenses may be a good choice for patients who have an elevation change exceeding 350 µm over an 8.0 mm chord of an elevation map,26 however it is important to remember that patient needs, lifestyle, and abilities also should be considered when choosing the ideal lens to fit for each individual.
While scleral lenses may serve a dual purpose in keratoconus patients with comorbid dry eye disease, outcomes may be adversely affected by allergies and atopy, which are common in this patient population.20,27 Handling and dexterity issues can further complicate scleral lens wear.
Other scleral lens fitting challenges in patients who have keratoconus include lens decentration, insufficient or excess central tear reservoir clearance, epithelial bogging, transition zone (limbal) bearing, conjunctival prolapse, peripheral curve/edge landing fit issues (eg, impingement/seal-off or lift-off), and lens complications due to overwear.28 To prevent these issues, the lens should be carefully assessed and modified during the fitting process and monitored on a regular basis at interim visits. At those follow-up visits, the lens fit should be evaluated after the lens has been on for 4 or more hours (to ensure proper settling), and then removed to evaluate the cornea underneath the lens with sodium fluorescein.
Because the thickness of both the lens and the post-lens fluid reservoir can theoretically decrease oxygen transmissibility through the lenses, patients should be monitored to ensure no corneal hypoxia, neovascularization, or endothelial cell loss develops as a result of lens wear with both baseline and periodic assessment of corneal pachymetry and specular microscopy.28
Challenges patients may experience with scleral lens wear include lens discomfort, fogging (front surface fogging and/or tear reservoir fogging), solution compliance, overwear, and discomfort (Figure 1). Patients who have dry eye, allergies, or atopy may be at higher risk for midday fogging.28 To relieve fogging and tear reservoir debris, ensure optimal treatment of comorbid ocular surface disease and allergy, such as an antihistamine-mast cell stabilizer drop in the morning prior to lens wear and periodic pulses of topical corticosteroids as needed.
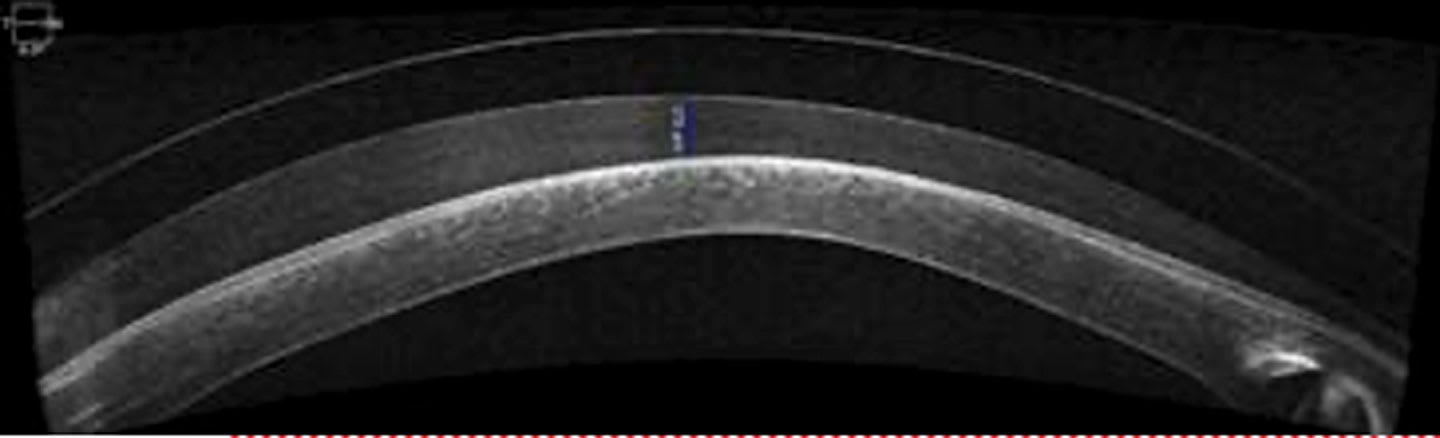
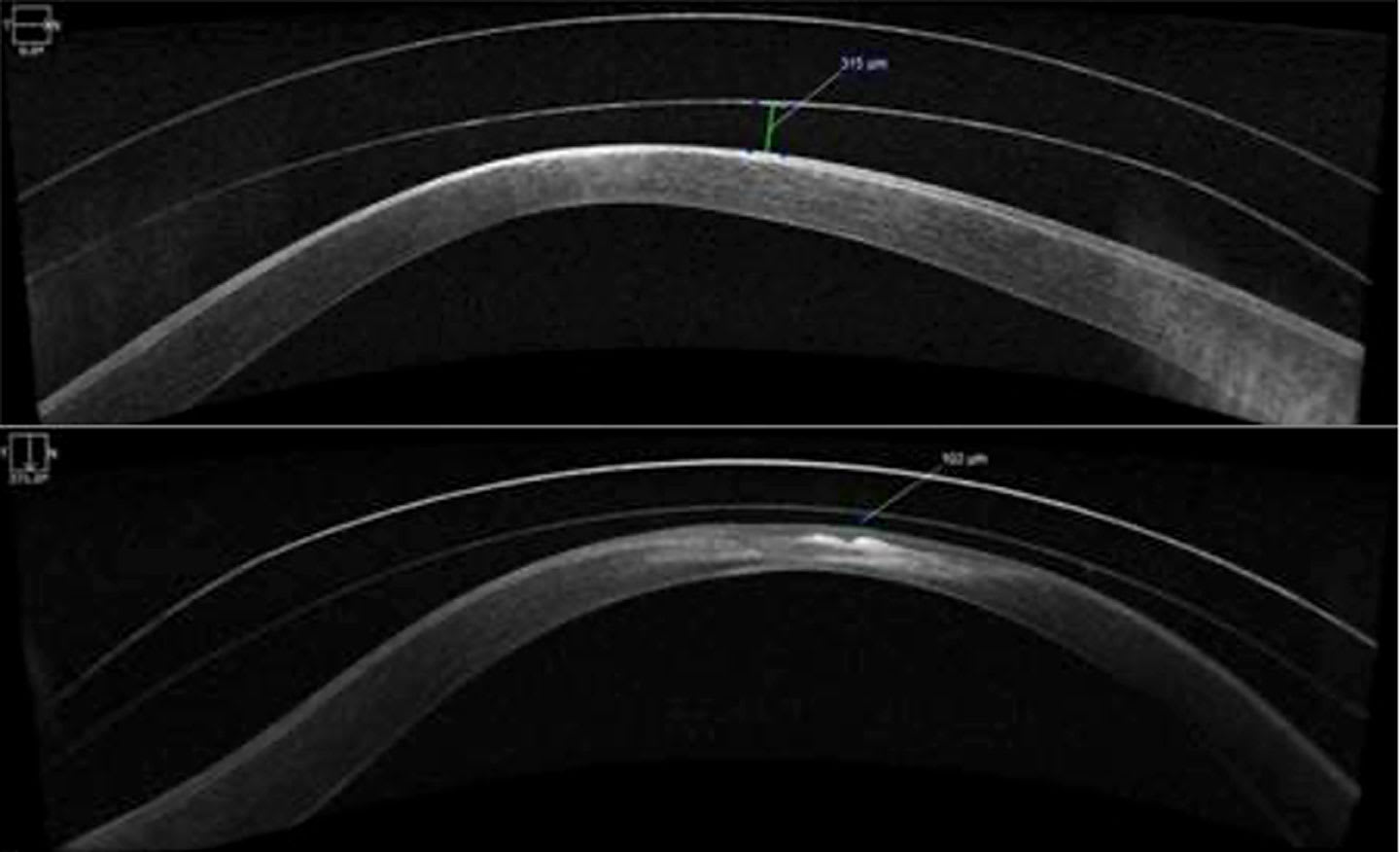
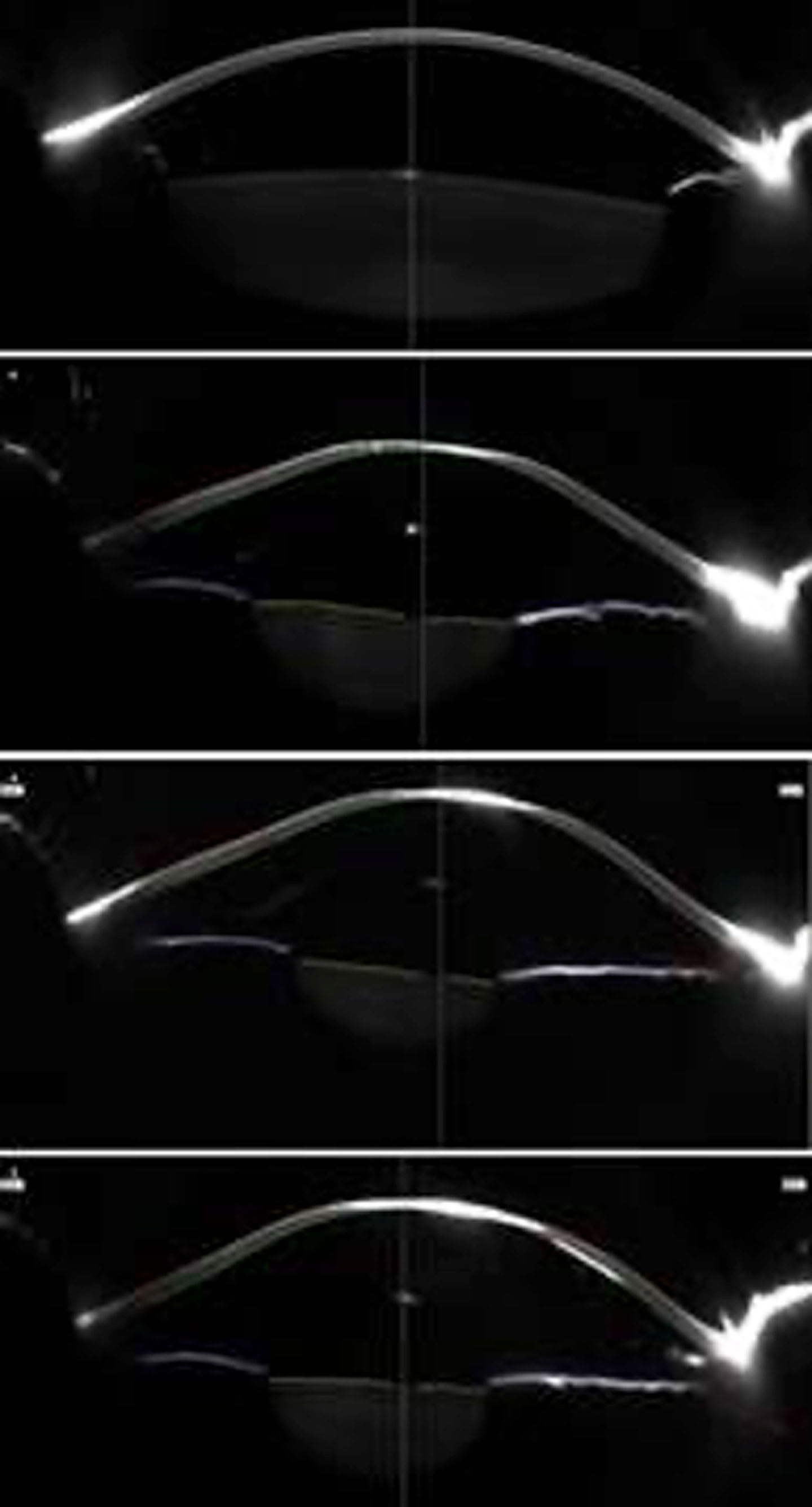
Ensure the fit is appropriate, with appropriate peripheral curve landing and the minimum possible apical clearance with the goal of achieving a fit with a plano tear layer.28 The goal of avoiding excess clearance can be impossible to achieve with standard corneal chamber designs on highly irregular corneas (Figure 2). Adding more viscous preservative-free artificial tears to the lens bowl doesn’t necessarily remove the debris, but it may keep it out of the visual axis and slow its formation.28 Patients may also opt for midday lens flushing with preservative-free saline or remove lenses midday and replenish the post-lens tear reservoir solution.
Recommendations for lens care solutions can vary depending on each patient’s unique circumstances or complications. In those patients who have discomfort, practitioners may elect to add plasma treatment or a PEG coating to the scleral lens or prescribe use of a preservative-free hydrogen peroxide-based system to prevent exacerbation of dryness and formation of deposits. For some wearers, it is advisable to suggest using a GP lens conditioning solution routinely in addition to a hydrogen peroxide-based system, to ensure the lens material’s wetting properties remain robust day-to-day.
Filling solutions are another consideration—options vary in pH, and they can be buffered or non-buffered. Most recently, patients have been navigating recalls of nonpreserved saline, and practitioners have been made aware of the potential dangers of generic nonpreserved saline solutions available on popular e-commerce platforms.26,29-31
Of course, for noncompliant patients, concerns about contact lens overwear and related complications remain. All keratoconus patients who wear contact lenses should be regularly advised on the symptoms of complications, including redness, eye pain, irritation, light sensitivity, and changes in vision. Recommendations for lens care and proper solutions should be reviewed at each office visit. Unfortunately, any contact lens-related complication in a keratoconus patient wearing medically necessary contact lenses can leave the patient with vision that is rendered non-functional, even with spectacles, affecting their work and home life in a significant way.
Emotional Support
Practitioners who frequently manage patients who have corneal ectasia can tell you story after story of patients they have seen for years and whose lives have been improved by scleral lenses. Eyecare practitioners serve as an emotional support for these patients who may be battling mental health challenges related to their chronic, progressive disease or simply the frustrations of contact lens wear, care, and handling. It is important to stress the need for compliance with prescribed solutions, periodic follow-up visits to assess vision, lens integrity, and lens fit, and to monitor for complications. With the onset of signs or symptoms of complications, including hydrops, patients should be aware of how to reach their provider’s office for urgent evaluation if needed.
Patient Case
A 16-year-old female patient presented with constant blurry vision at distance in both eyes that was worse at night ongoing for the past 3 months. She noted associated headaches and photophobia and did not wear glasses. As a junior in high school, her near work was extensive and she was managing to get As and Bs.
Entering visual acuity was OD 20/70 and OS 20/25. Refraction was OD –3.00 –1.00 x 070, 20/25 and OS –1.25 –1.00 x 090, 20/20. Slit lamp examination revealed mild apical thinning and a Fleisher ring in each eye. Intraocular pressure was 15 mmHg in each eye, and the dilated fundus evaluation was within normal limits in each eye.
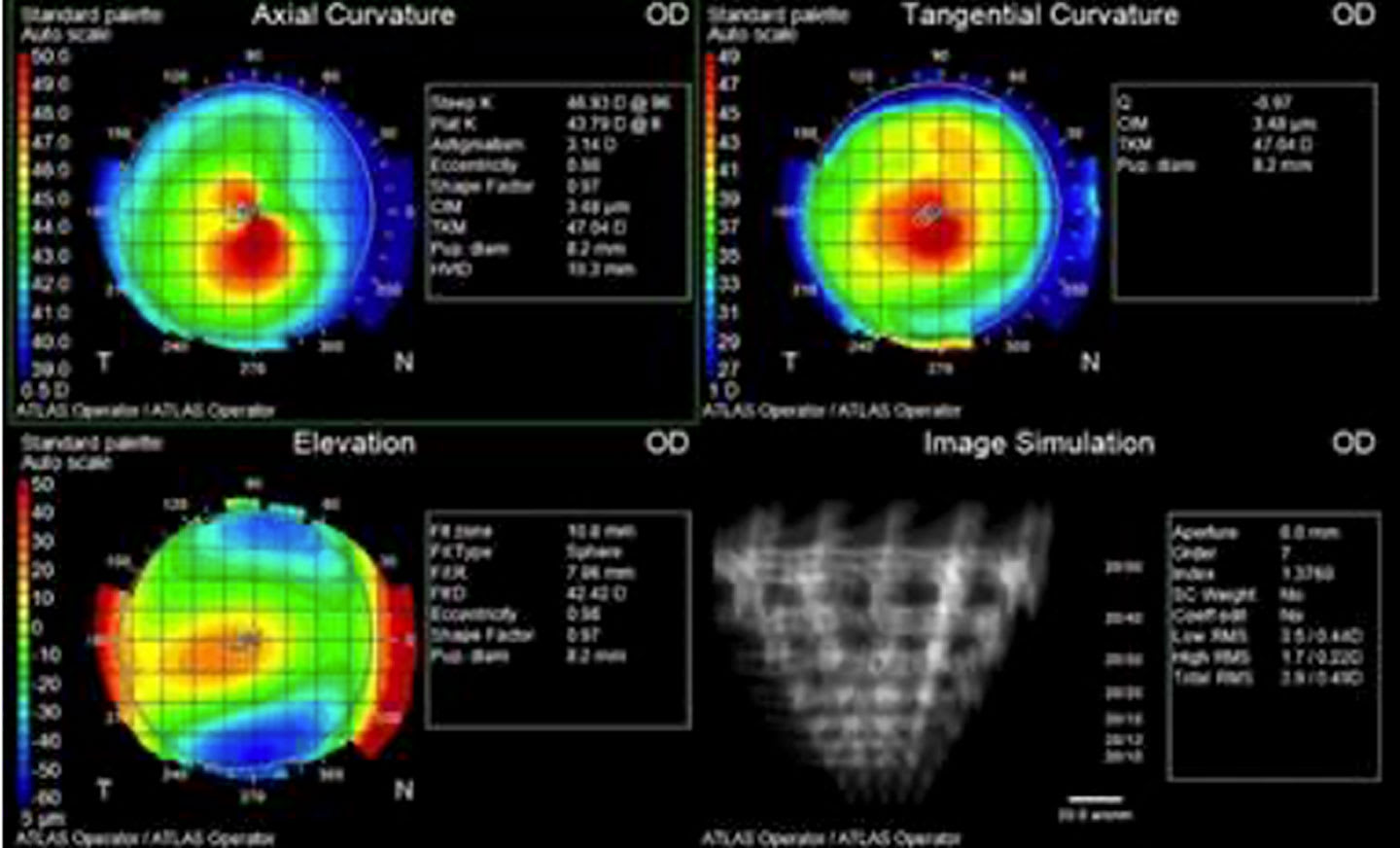
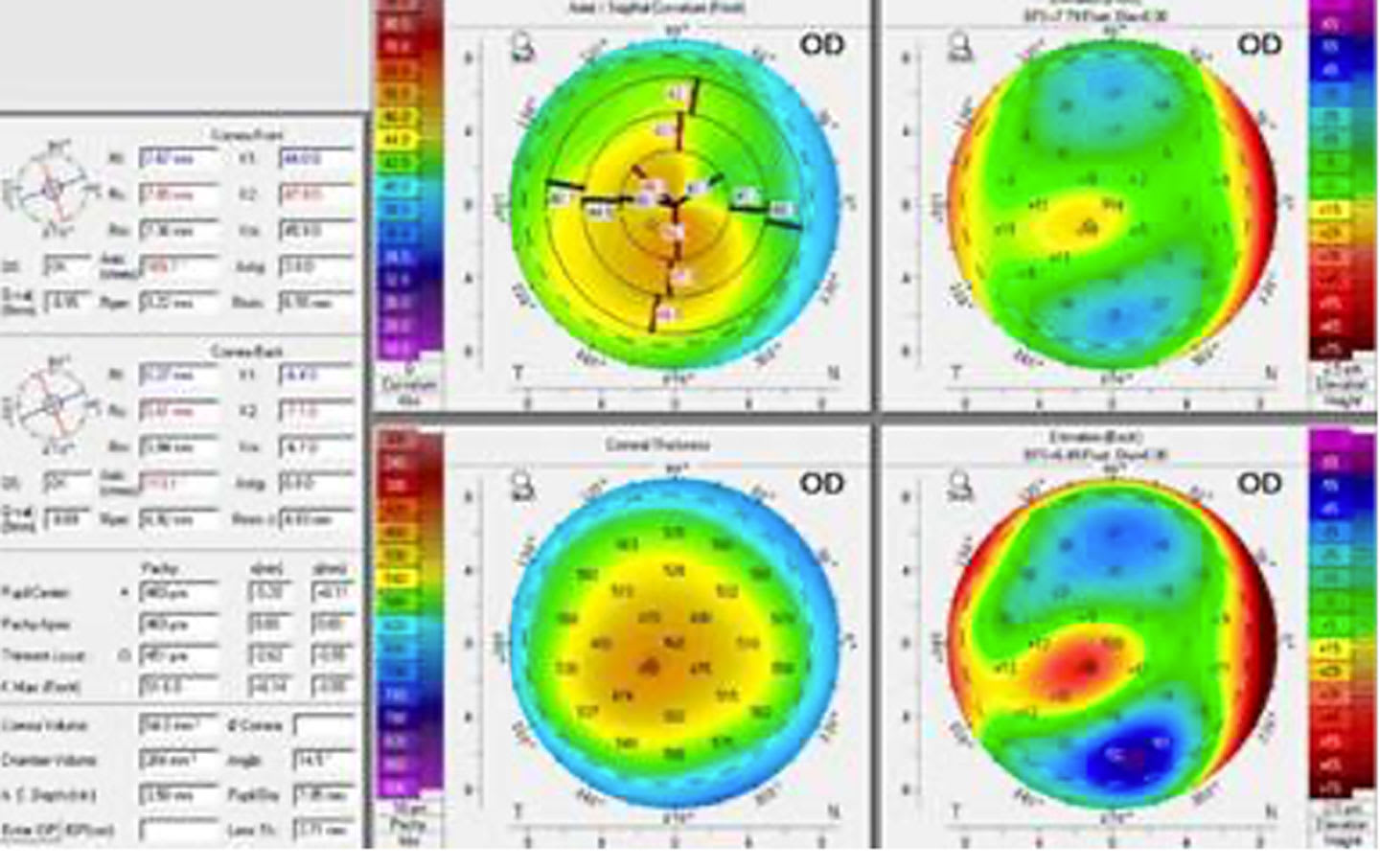
The patient underwent corneal topography (Figure 3) which was deemed suspicious and so tomography was also obtained (Figure 4). Simulated keratometry readings from the topography map were OD 43.79/46.93@096 and OS 43.38/46.31@084. The Belin-Ambrosio enhanced ectasia map confirmed the presence of ectasia with an abnormal BAD-D value of 6.26 (Figure 5a). The patient elected to proceed with spectacle lens wear, given the drastic improvement in visual acuity gained by refraction at this visit.
The patient returned more than 2 years later with a complaint of gradually progressive blurry vision, relieved by holding her devices very close to her eyes. She reported she was doing well in school and would be going to college in the fall.
She been to a different provider for eye care 1 year prior and got new glasses. Entering vision with the habitual lenses was OD 20/400 and OS 20/400. The habitual spectacle prescription was OD –3.50 –1.25 x 075 and OS –1.25 –1.25 x 085, and no improvement in visual acuity was achieved with manifest refraction. Tomography imaging revealed simulated keratometry readings of OD 61.20/70.60@096 and OS 52.90/56.60@090. The minimum pachymetry readings were OD 369 µm and OS 408 µm. At this time, CXL was recommended, but the patient could not undergo the procedure due to cost. Instead, she was fit in scleral contact lenses for vision improvement. The final lens parameters were OD 7.50 mm base curve (BC)/16.8mm diameter/–4.00 DS and OS 7.50 mm BC/14.8 mm diameter/+1.50 DS with quadrant-specific limbal and edge customization for each.
Multiple visits occurred each year for the next few years, and the patient was subsequently refit into duplicate lenses, lenses with prescription changes, and, eventually, larger-diameter scleral lenses to improve lens vault, comfort, and vision. The patient was 22 years old at the last stable visit and had simulated keratometry readings of OD 56.00/63.10@060 and OS 73.90/79.80@107. The minimum pachymetry readings were OD 233 µm and OS 383 µm. The most recent lens parameters were OD 6.69 mm BC, 15.6mm diameter, 4,850 sag height, and –9.50 DS and OS 7.18 mm BC, 15.6 mm diameter, 4,550 sag height, and –6.37 DS with a quadrant-specific midperipheral and limbal zone in each eye and a toric landing zone in each eye. The lenses were manufactured using a 100 Dk lens material with a polyethylene glycol (PEG)-based coating. Visual acuity with the lenses was OD 20/30 and OS 20/40.
Then, at 23 years old, the patient presented for an urgent evaluation of a red, painful, right eye upon waking 2 days prior. She presented to a local hospital emergency room and was prescribed erythromycin ointment every 2 hours before presenting to our clinic. Entering visual acuity was hand motion OD without correction and 20/60 OS with scleral lens correction.
Slit lamp examination revealed significant corneal edema with microcystic edema overlying OD. New apical corneal scarring was noted OS that was likely affecting the best-corrected vision in that eye. AS-OCT imaging confirmed the presence of a Descemet membrane break, and the diagnosis of acute corneal hydrops in the right eye was made. The intraocular pressure was measured at 5 mmHg.
Treatment was initiated with 5% sodium chloride ointment 6 times daily in each eye, doxycycline 50 mg by mouth twice daily, and vitamin C 1,000 mg by mouth daily. To manage pain, 1 drop of cyclopentolate 1.0% was instilled in the office OD. Acetaminophen alternating with ibuprofen was recommended for pain management. The patient was given a note for her work, in hopes that they would make accommodations due to the significant eye pain and light sensitivity.
As the hydrops improved (slowly) over the next several months, vision in the right eye improved to 20/400, then 20/100, and finally to 20/50 with a new scleral lens fit following resolution. Vision in the left eye remained stable at 20/50 with a new scleral lens.
At the last stable visit, the patient had simulated keratometry readings of OD 63.60/69.40@047 and OS 74.60/80.60@050. The minimum pachymetry readings were OD 253 µm and OS 337 µm. The BAD-D value was not able to be calculated due to the high level of irregularity (Figure 5b).
The most recent lens parameters were OD 6.70 BC, 14.3 diameter, 4,850 sag height , and –9.37 DS and OS 7.00 BC, 14.9 diameter, and –7.62 DS with a quadrant-specific limbal zone in each eye and a toric landing zone in each eye. The lenses were manufactured in 200 Dk lens material with a PEG-based coating.
This patient exemplifies the varied needs of keratoconus patients over time and shows the marked progression of the corneal steepening and thinning over time. (Figure 6). In this young patient who could not obtain cross-linking, the progression required large changes in the scleral lens fitting parameters when comparing the initial fit (Figure 2A) to the most recent fit (Figure 2B). Steepening, thinning, scarring, and irregularity of the corneas increased over the course of five years of lens wear, and included an episode of hydrops.
Through all of this, the patient has remained compliant with treatment and follow-up visits and was excited that her post-hydrops vision had improved so she could return to work. Her final scleral lens was noted as the most comfortable lens she has ever worn, and she is considering a future corneal transplant in the right eye. For now, we are hopeful we can delay for as long as possible, while hoping hydrops does not occur in the left eye. Fortunately, if hydrops occurs in the left eye, the patient will be well-versed in its symptoms.
Acknowledgments: The author would like to acknowledge William Tullo, OD, for his expertise in tomography and Sarah Chung, OD, for her collaboration in the management of the hydrops patient presented.
References
-
Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol. 1984;28(4):293-322. doi:10.1016/0039-6257(84)90094-8
-
Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297-319. doi:10.1016/s0039-6257(97)00119-7
-
Harthan JS, Gelles JD, Block SS, et al. Prevalence of keratoconus based on Scheimpflug corneal tomography metrics in a pediatric population from a Chicago-based school age vision clinic. Eye Contact Lens. 2024;50(3):121-125. doi:10.1097/ICL.0000000000001072
-
Belin MW, Harthan JS, Eiden SB, et al. Revised calculation of the prevalence of keratoconus based on updated scheimpflug corneal tomography metrics in a pediatric population from a Chicago-based school age vision clinic. Eye Contact Lens. 2026;52(3):103-104. doi:10.1097/ICL.0000000000001250
-
Kymes SM, Walline JJ, Zadnik K, Gordon MO, Collaborative Longitudinal Evaluation of Keratoconus study group. Quality of life in keratoconus. Am J Ophthalmol. 2004;138(4):527-535. doi:10.1016/j.ajo.2004.04.031
-
Steinberg J, Fischer P, Frings A, Druchkiv V, Katz T, Linke SJ. Quality of life in patients with progressive keratoconus treated with corneal collagen crosslinking. Int Ophthalmol. 2025;45(1):103. doi:10.1007/s10792-024-03400-6
-
Panthier C, Moran S, Bourges JL. Evaluation of vision-related quality of life in keratoconus patients, and associated impact of keratoconus severity indicators. Graefes Arch Clin Exp Ophthalmol. 2020;258(7):1459-1468. doi:10.1007/s00417-020-04680-1
-
Durakovic E, Kandel H, Watson SL. Mental health impact of keratoconus: A systematic review. Cornea. 2023;42(9):1187-1197. doi:10.1097/ICO.0000000000003263
-
Fan L, Kandel H, Watson SL. Impacts of keratoconus on quality of life: a qualitative study. Eye (Lond). 2024;38(16):3136-3144. doi:10.1038/s41433-024-03251-6
-
Lim L, Lim EWL. Current perspectives in the management of keratoconus with contact lenses. Eye . 2020;34(12):2175-2196. doi:10.1038/s41433-020-1065-z
-
Nau CB, Harthan JS, Shorter ES, et al. Trends in scleral lens fitting practices: 2020 Scleral Lenses in Current Ophthalmic Practice Evaluation survey. Eye Contact Lens. 2023;49(2):51-55. doi:10.1097/ICL.0000000000000960
-
Schornack MM, Nau CB, Harthan J, Shorter E, Nau A, Fogt J. Current trends in scleral lens prescription, management, and evaluation. Eye Contact Lens. 2023;49(2):56-62. doi:10.1097/ICL.0000000000000957
-
Gomes JAP, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359-369. doi:10.1097/ICO.0000000000000408
-
Matalia H, Swarup R. Imaging modalities in keratoconus. Indian J Ophthalmol. 2013;61(8):394-400. doi:10.4103/0301-4738.116058
-
Souza Oliveira R, Gil JQ, Rosa A, Quadrado MJ, Campos M. Keratoconus detection in high-astigmatism pediatric patients: Optimal Pentacam indices and cutoff points. Cornea. 2025;44(12):1521-1527. doi:10.1097/ICO.0000000000003755
-
Wu D, Hong J, Wu S, Xu J. Corneal topography parameters and tear film break-up characteristics in keratoconus patients. Br J Hosp Med (Lond). 2025;86(7):1-16. doi:10.12968/hmed.2024.0825
-
Sari D, Kandel H, Kha R, Watson SL. What is the quality-of-life status of patients with keratoconus who have not had a surgical intervention? A systematic review. Eye (Lond). 2025;39(18):3229-3236. doi:10.1038/s41433-025-04053-0
-
Vincent SJ, Alonso-Caneiro D, Collins MJ. Optical coherence tomography and scleral contact lenses: clinical and research applications: OCT and scleral contact lenses. Clin Exp Optom. 2019;102(3):224-241. doi:10.1111/cxo.12814
-
Debourdeau E, Planells G, Chamard C, et al. New keratoconus risk factors: A cross-sectional case-control study. J Ophthalmol. 2022;2022:6605771. doi:10.1155/2022/6605771
-
Seth I, Bulloch G, Vine M, et al. The association between keratoconus and allergic eye diseases: A systematic review and meta-analysis. Clin Experiment Ophthalmol. 2023;51(4):O1-O16. doi:10.1111/ceo.14215
-
Gordon-Shaag A, Millodot M, Shneor E, Liu Y. The genetic and environmental factors for keratoconus. Biomed Res Int. 2015;2015:795738. doi:10.1155/2015/795738
-
Bawazeer AM, Hodge WG, Lorimer B. Atopy and keratoconus: a multivariate analysis. Br J Ophthalmol. 2000;84(8):834-836. doi:10.1136/bjo.84.8.834
-
McMonnies CW. Mechanisms of rubbing-related corneal trauma in keratoconus. Cornea. 2009;28(6):607-615. doi:10.1097/ICO.0b013e318198384f
-
Jones-Jordan LA, Walline JJ, Sinnott LT, Kymes SM, Zadnik K. Asymmetry in keratoconus and vision-related quality of life. Cornea. 2013;32(3):267-272. doi:10.1097/ICO.0b013e31825697c4
-
Kandel H, Nguyen V, Piermarocchi S, et al. Quality of life impact of eye diseases: a Save Sight Registries study. Clin Experiment Ophthalmol. 2022;50(4):386-397. doi:10.1111/ceo.14050
-
Zheng F, Caroline P, Kojima R, Kinoshita B, Andre M, Lampa M. Corneal elevation differences and the initial selection of corneal and scleral contact lens. Presented at: Global Specialty Lens Symposium; January 2015; Las Vegas, NV.
-
Hashemi H, Heydarian S, Hooshmand E, et al. The Prevalence and Risk Factors for Keratoconus: A Systematic Review and Meta-Analysis. Cornea. 2020;39(2):263-270. doi:10.1097/ICO.0000000000002150
-
Walker MK, Bergmanson JP, Miller WL, Marsack JD, Johnson LA. Complications and fitting challenges associated with scleral contact lenses: A review. Cont Lens Anterior Eye. 2016;39(2):88-96. doi:10.1016/j.clae.2015.08.003
-
US Food and Drug Administration. FDA Class 2 Device Recall: Nutrifill. Accessed March 4, 2026. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfres/res.cfm?id=213989
-
Petris R, Moore A, Brown S. Unsafe E-Commerce Marketing of Contact Lens Solutions. Presented at: Global Specialty Lens Symposium; January 2025; Las Vegas, NV. Accessed March 4, 2026. https://gslsymposium.com/live/3/page/120?poster_id=247
-
Moore A, Petris R, Brown S. Unsafe Scleral Lens Filling Solutions Sold on Amazon are Putting Patients at Risk. Presented at: Global Specialty Lens Symposium; January 2026. Accessed March 4, 2026. https://gslsymposium.com/live/3/page/119?poster_id=710