



The image shows Munson’s sign, reflecting an advanced stage of keratoconus in this case, wearing an intralimbal GP lens in his left eye.
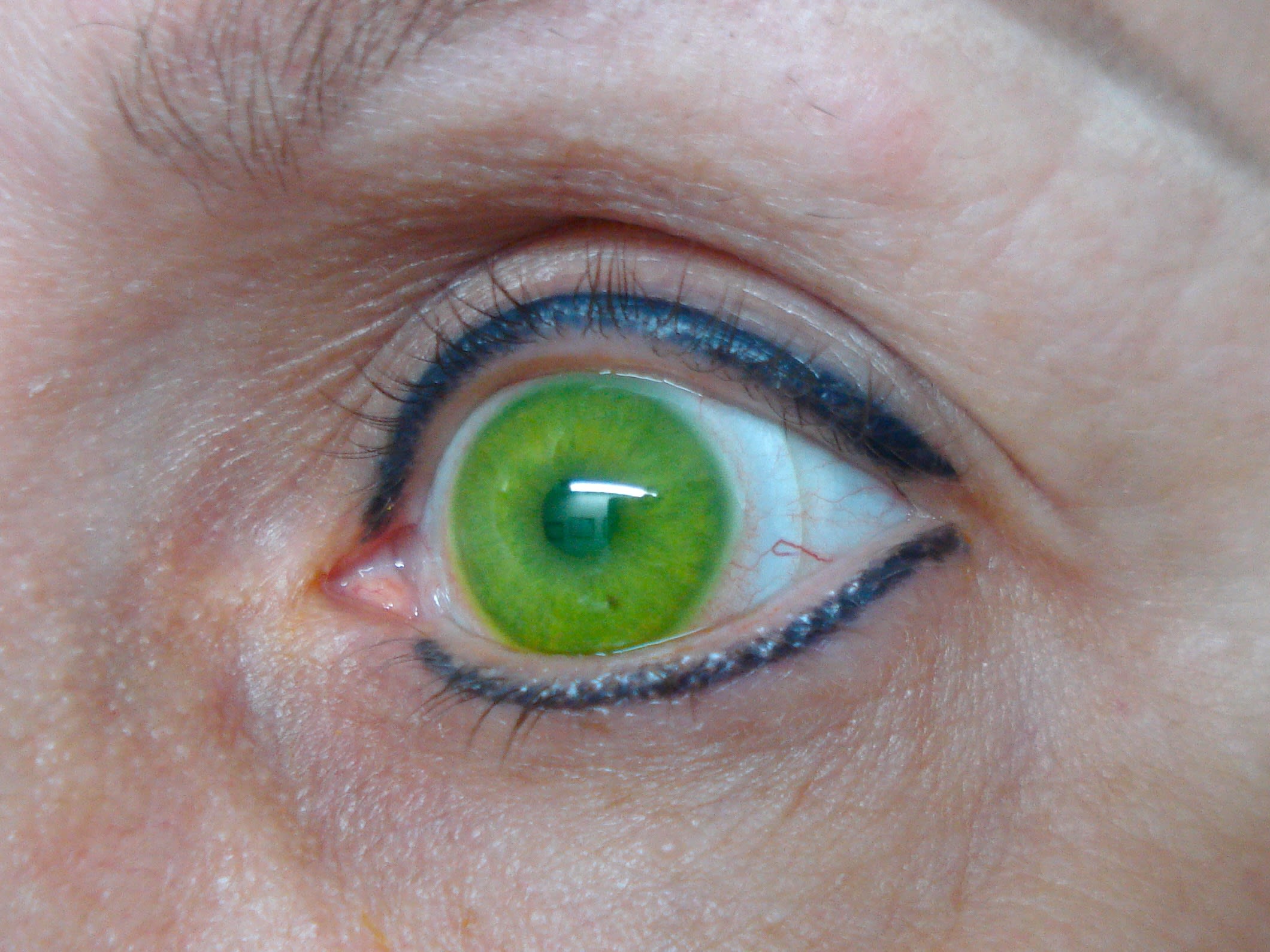
At her first examination in 1997, the patient presented with toxoplasmosis, amblyopia, and central corneal scarring in her right eye. She was fit with a specialized bicurve rigid gas permeable lens designed specifically for managing keratoconus OS. In 2011, she was refit with large intralimbal GPs in both eyes. Although the right eye had no central vision due to toxoplasmosis, amblyopia, and advanced keratoconus, the patient benefited from improved functional peripheral vision, especially temporally (Figure 2).

Clinical Challenge
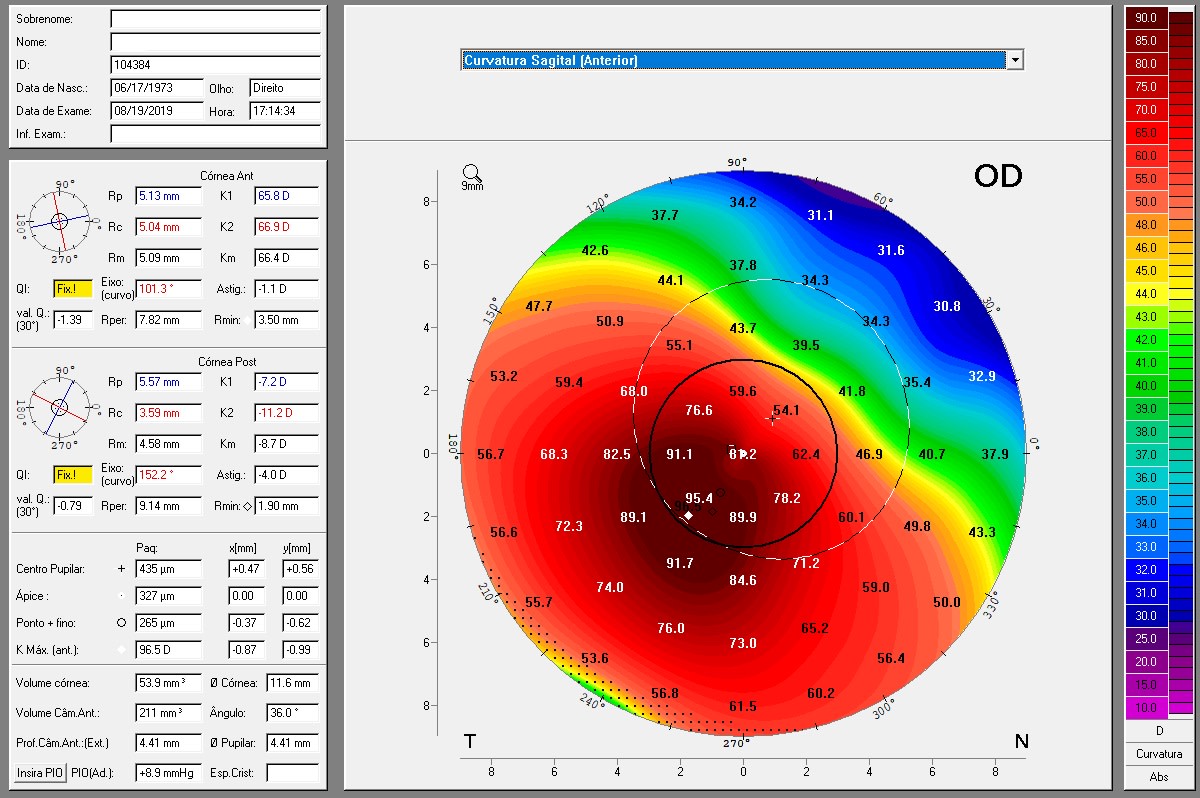
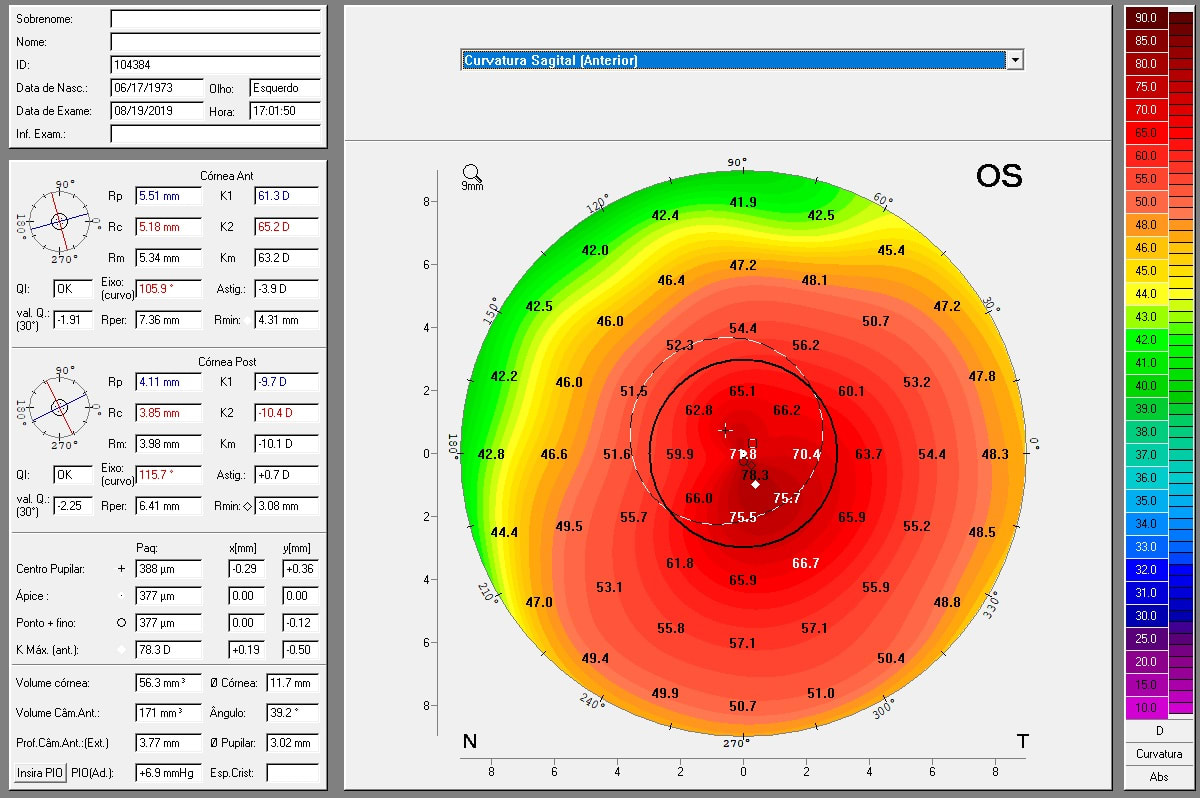
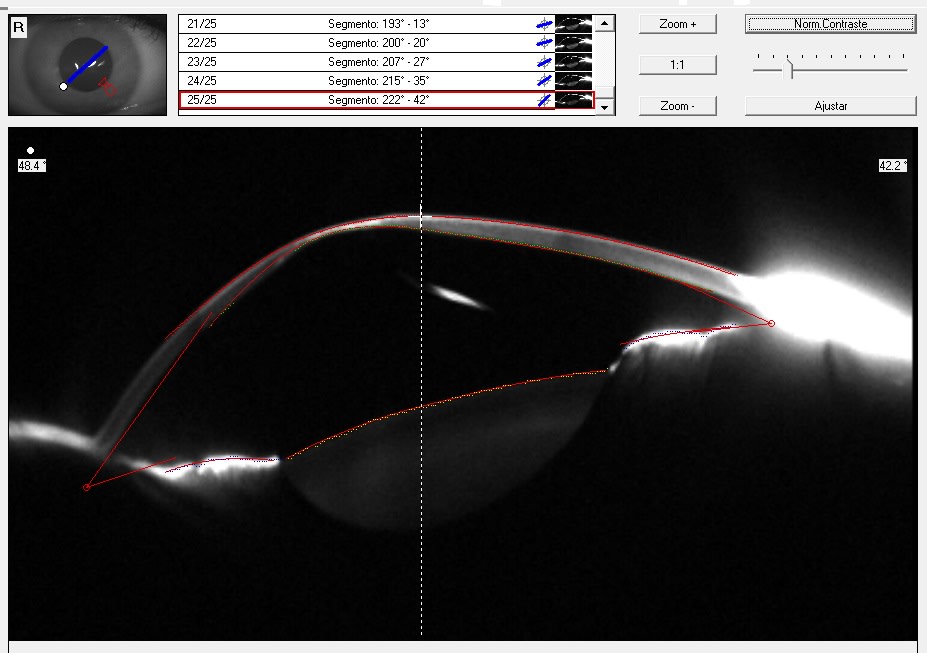
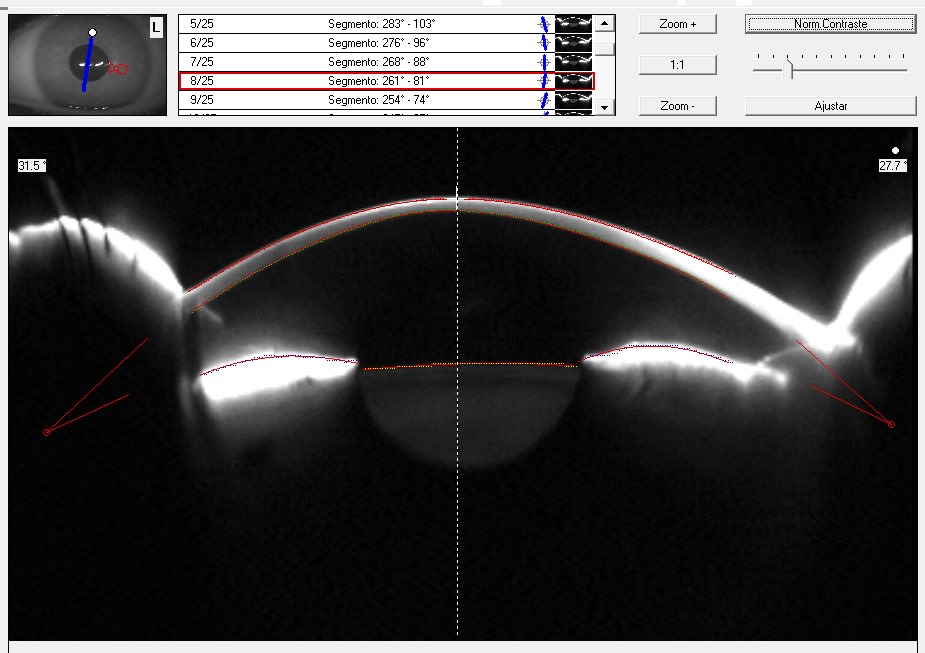
Corneal tomography and Scheimpflug images (Figures 3, 4, 5, and 6) show the severe stage of her keratoconus, especially OD. An intralimbal GP design was fit so she could benefit from functional vision (temporal) in the right eye and her resulting acuity in the left eye was 20/60+3/J-4. The lenses provided stability and tear exchange, corneal physiological health was maintained, and the patient reported comfortable lens wear.
The intralimbal GP lens parameters were:
OD: 74x48 D base curves, –32.5 D power, 11.5 mm overall diameter (OAD), 7.5mm optic zone (OZ), a Dk of 100, (peripheral vision)
OS: 62x45 D base curves, -16.5 D power, 11.5mm OAD, 7.0 mm OZ, a Dk of 100 and a visual acuity of 20/60
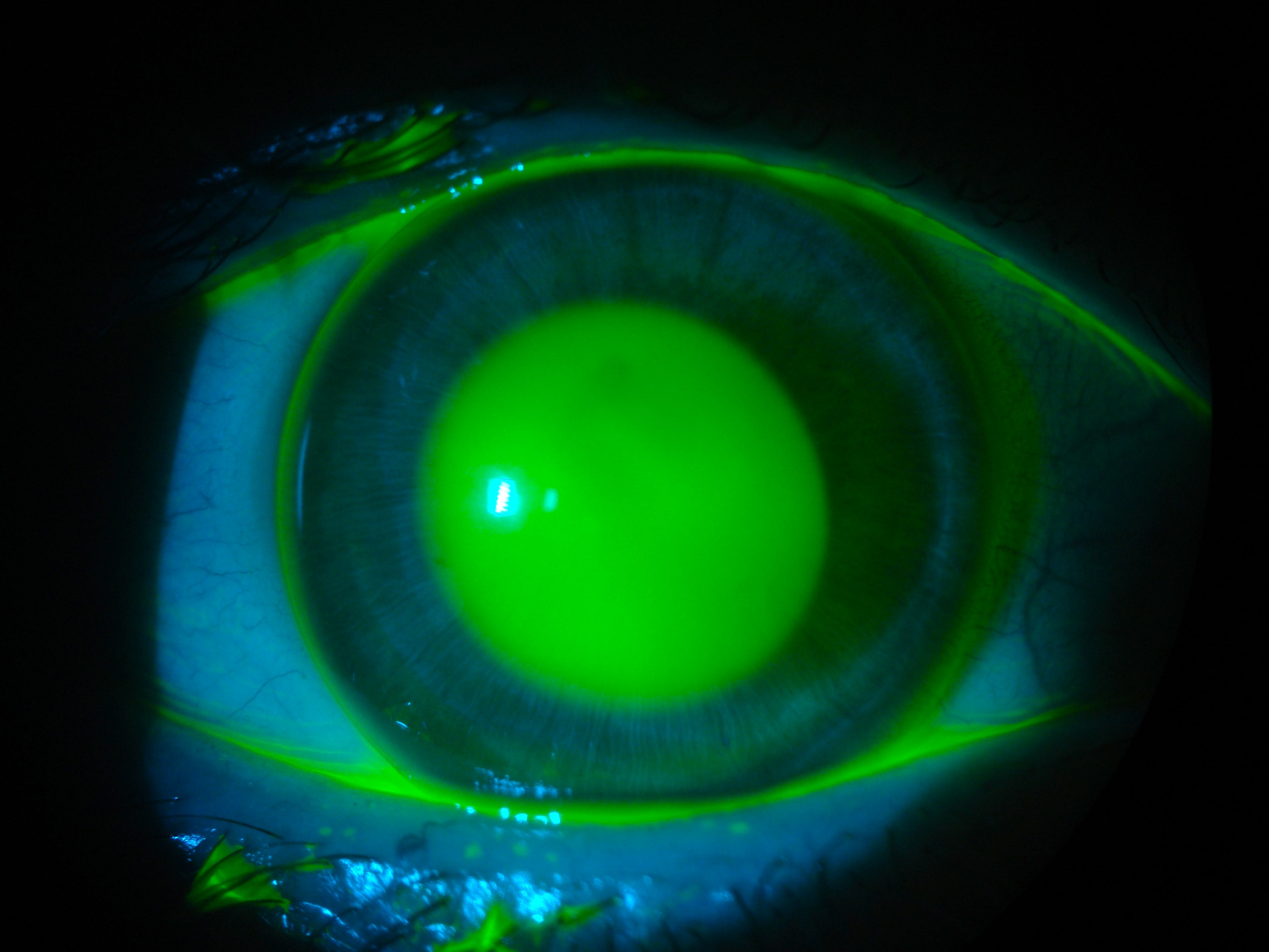
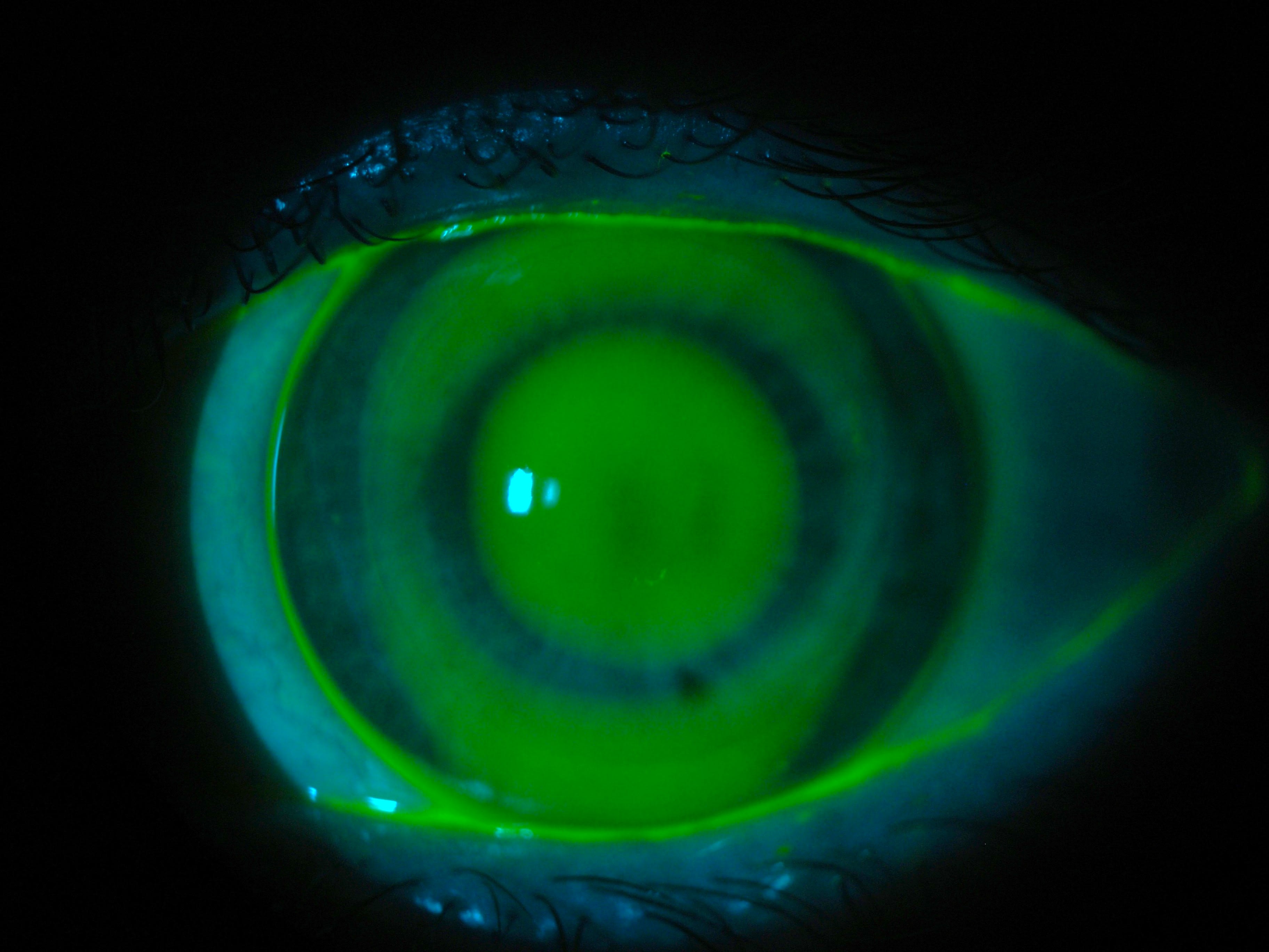
Minor adjustments were made to the lens periphery to increase tear exchange and maintain corneal physiological health. (Figures 7 and 8).
The motivation to fit her right eye despite absence of central vision was found when the patient perceived an improvement in peripheral vision. The over-refraction was performed using certificates on the wall as a target for this eye The patient could describe when the frames appeared sharper during the exam.
The patient was glad that she partially recovered some vision OD.
In 2019 during a follow-up visit, contact lens wear was determined to be contraindicated OD due to extremely low corneal pachymetry and increased risk to corneal integrity. At this time, OS was refitted with a scleral lens (Figure 9).
Conclusion
This case shows a timeline of technological evolution that helped achieve the best possible vision over the last decades. From corneal GP designs for keratoconus to intralimbal lenses and, more recently, scleral lenses.
Today, with modern scleral designs and materials, practitioners can explore more functional vision even in eyes that have poor central acuity. Often patients benefit from improved peripheral vision with these lenses and, therefore, feel more confident of their surroundings.
Related Reading
1. Lapum JL, Hughes M, eds. Introduction to Health Assessment for the Nursing Professional. Canadian ed. Chapter 17, Ophthalmic System Assessment – The Eyes. 2024
2. Yun E. Central Vision vs Peripheral Vision. Oxsight. January 17, 2024. https://www.oxsight.co.uk/news/central-vision-vs-peripheral-vision
3. Wolfe B, Dobres J, Rosenholtz R, Reimer B. More than the Useful Field: Considering peripheral vision in driving. Appl Ergon. 2017;65:316-325. doi: 10.1016/j.apergo.2017.07.009
4. McLain R. Peripheral vision and what we can see in the dark. Science News Explore. 2024. https://www.snexplores.org/article/peripheral-vision-and-what-we-can-see-in-the-dark
5. Brookshire B. Teen researcher eyes peripheral vision. Science News Explore. 2015.https://www.snexplores.org/blog/eureka-lab/teen-researcher-eyes-peripheral-vision
6. Carr JN, Johnson CA. Visual Field Testing: From One Medical Student to Another. The University of Yowa – Department of Ophthalmology and Visual Sciences.
https://eyerounds.org/tutorials/VF-testing/#gsc.tab=0