


SCLERAL LENSES can correct higher-order aberrations (HOAs) by masking front-surface corneal irregularity. Unfortunately, some patients have additional HOAs from the posterior cornea, phakic lens, or vitreous that can limit best-corrected visual acuity. The case presented here highlights a patient who had corneal ectasia and was able to achieve improved visual acuity with a scleral lens that included wavefront optics to correct for residual HOAs.
This 52-year-old female had a history of post-laser-assisted in situ keratomileusis (LASIK) surgery, resultant corneal ectasia, and post-corneal cross-linking of both eyes. She came in complaining of decreased vision without significant improvement with glasses correction. Manifest refraction and visual acuities were +2.50 –0.25 x 045 20/300 OD and +0.50 –2.25 x 045 20/300 OS. Scheimpflug imaging showed severe front- and back-surface corneal ectasia in both eyes.
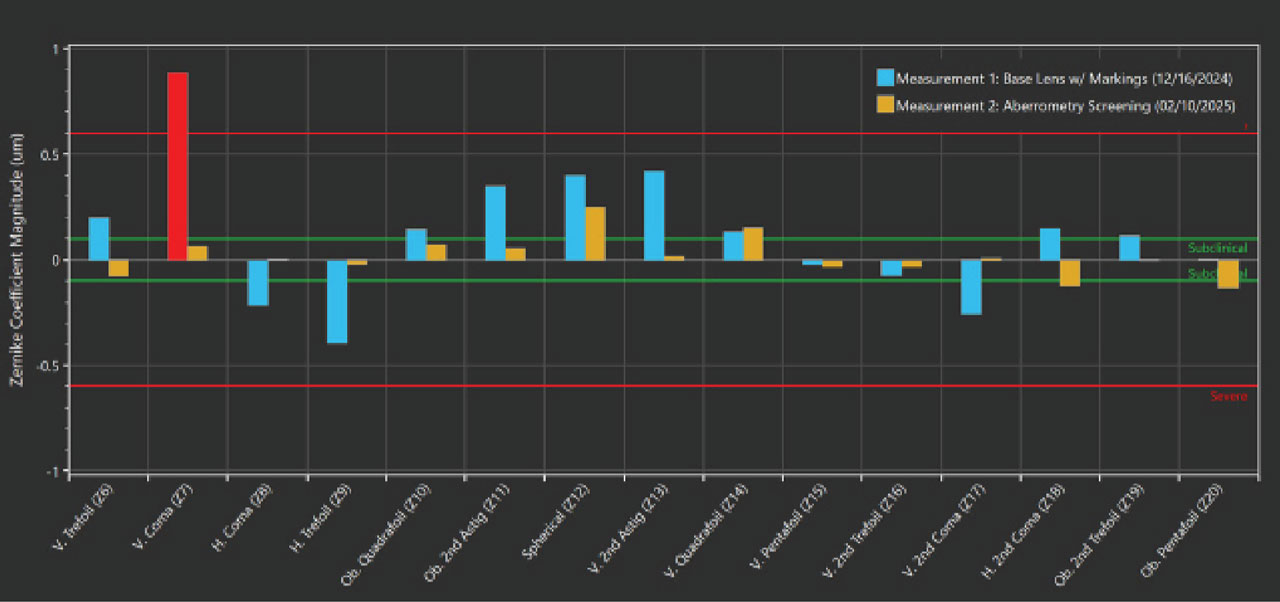
The patient was referred for scleral lens fitting. She was fit with 16.5 mm scleral lenses with customized back-surface landing zones of –8.50 20/40 OD and–7.93 20/40 OS. Although the scleral lenses provided significant improvement in visual acuity, the patient subjectively reported poor vision while wearing them. Hartmann-Shack aberrometry measurements over the scleral lenses revealed significant residual HOAs, including high amounts of positive vertical coma (Figure 1), secondary to her highly irregular posterior corneal surface.

Scleral lenses were redesigned with a front-surface eccentricity value of –0.6. It has been demonstrated that front-surface eccentricity can reduce residual HOAs, including coma (Hussoin et al, 2025). The dispensation of those lenses resulted in visual acuities of 20/60 OD and 20/100 OS. Overaberrometry measurements showed no reduction in positive vertical coma, which is one of the most debilitating HOAs.
After failure with front-surface aspheric correction, scleral lenses were ordered with front-surface wavefront correction customized to correct for her residual HOAs. The lens optics were decentered to match over the patient’s pupil. With the wavefront-corrected scleral lenses, the patient was able to see 20/25 in each eye, and she reported significant subjective visual improvement. Overaberrometry measurements revealed reduced residual HOAs (Figure 2).
A recent paper evaluated wavefront-corrected scleral lenses vs traditional scleral lenses for 18 patients, the majority of whom had corneal ectasia. The research indicated that the wavefront-corrected scleral lenses improved higher-order root-mean-square values by 56% (Gelles et al, 2025). Seventeen of the 18 patients subjectively preferred the scleral lenses with wavefront correction vs the traditional scleral lenses.
Patients who have corneal ectasia are often left with suboptimal visual acuity despite wearing successfully fit scleral lenses with standard optics. The issue for these patients is that they often have significant back-surface corneal irregularity that results in residual positive vertical coma. Front-surface eccentricity can reduce residual HOAs for some patients, but in this case, it actually worsened her visual acuity. Customized wavefront correction was the solution that allowed her to have improved visual function. In some cases, neural adaptation to the wavefront correction is required to achieve subjective satisfaction.
References
1. Hussoin T, Le HG, Carrasquillo KG, et al. The effect of optic asphericity on visual rehabilitation of corneal ectasia with a prosthetic device. Eye Contact Lens. 2012;38(5):300-305. doi: 10.1097/ICL.0b013e3182657da5
2. Gelles JD, Su B, Kelly D, et al. Visual improvement with wavefront-guided scleral lenses for irregular corneal astigmatism. Eye Contact Lens. 2025;51(2):58-64. doi: 10.1097/ICL.0000000000001152