

Many long-term gas permeable (GP) lens wearers struggle with discomfort, lens dislodgement, and unsatisfactory near vision as their ocular needs evolve. The case report presented in this article highlights how integrating multifocal scleral lenses can deliver improved comfort, stability, and functional vision for patients dissatisfied with corneal GPs.
Case Description
A 53-year-old male patient presented to our clinic for a specialty contact lens evaluation after being referred by his cornea specialist for an updated fit. The patient has an ocular history of keratoconus in both eyes, dry eye disease, and asthma. He had a history of RGP contact lens use for 25 years. The patient had issues with dry eye spells that caused the contact lens to pop out of his eye, and sports activities often caused dislodgement of the lens. He used over-the-counter reading glasses +1.75 for all near work and described overall disappointment in his reading vision.
Upon conversing with the patient, we learned that he was seeking a lens option that provided similar optical quality to GPs with better stability, and he did not want to use reading glasses. After completing tomography scans and refraction, we determined that a scleral lens was the best option. The manifest refraction measured at -2.25 -5.25 @ 084 and 0.00 -1.75 @ 090 with a visual acuity of 20/40 OD and 20/30 OS with glare.
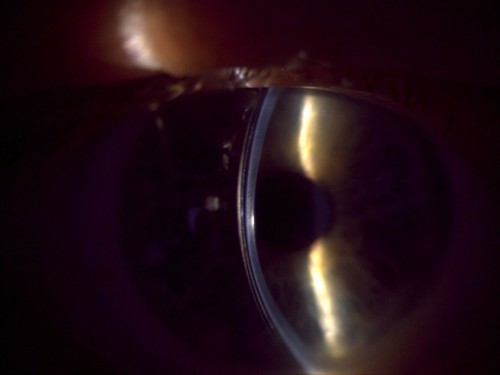
A scleral lens was applied to both eyes as a trial, and the patient noted immediate improvement in comfort and stability. Mild posterior tear film debris was caused by inferior lens decentration in both eyes. With the quadrant-specific haptics in the lens design, minor changes were instilled to improve comfort and fogging issues. We then completed an over-refraction and demonstrated a +1.50 for reading power, and the patient read J1.
At the original consultation, we chatted in depth about the potential for multifocal scleral lenses. The patient was informed about the potential limitations and adaptation of multifocal scleral lenses, and we decided to proceed. The choice for the multifocal design was a SmartFocus lens (BostonSight). We ordered the lenses after finalizing a stable fit and then dispensed the lenses.
When the patient returned to the clinic for follow-up, he reported that he was extremely pleased with the comfort that the lenses provided. However, he felt that his eyes were still adapting to the multifocal lenses. He was having difficulty at near distances, but his intermediate distance vision seemed great. We adjusted the lenses by adjusting the near optical zone.
Discussion
To aid in the adaptation for near work, a couple of options are available to improve vision. First, conversing with the patient about the adaptation time frame of a new multifocal lens is paramount. Once neuroadaptation occurs, multiple steps can be taken to improve near visual acuity.
Manipulating the effective near zone within this novel multifocal lens design allowed for improvements in near vision without distorting the distance vision. This change was due to the patient not having any issues with distance vision.
Conclusion
At the 2-month follow-up, the patient was doing wonderful with a comfortable, stable scleral lens. The best visual acuity was found to be 20/20-2 OD/OS, J3 at intermediate, and J1 at near.

To hear Dr. Helin discuss this case, click here.