

Scleral lenses are increasingly recognized as a valuable tool in managing complex refractive conditions in pediatric patients, as the lenses can offer improved visual acuity and correction of astigmatism and myopia.
Case Description
A 6-year-old female patient with high astigmatism, possible bilateral amblyopia, and progressive myopia was referred by her pediatric ophthalmologist for a contact lens evaluation 1 month after successful 0.05% atropine therapy.
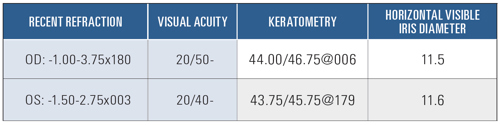
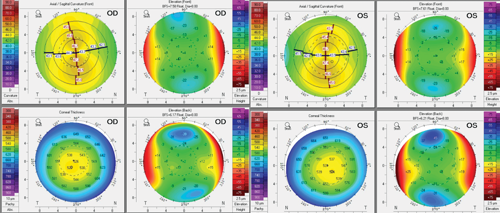
Ocular health assessment was normal. Topography was normal in both eyes exhibiting regular astigmatism and no evidence of keratoconus (see Figure 1). After several designs were rejected, due to either comfort or vision concerns, SynergEyes VS scleral lenses (CooperVision) were chosen.
The diagnostic lenses were: 3,600 µm sagittal depth (SAG)/8.4 mm base curve (BC)/plano/16.0 mm diameter (DIA)/Toric Landing Zones 36/42. The landing zone was adjusted to align better to the sclera. The central clearance was reduced to achieve 200 µm of central clearance. The base curve was steepened to reduce the limbal clearance
The lens diameter was increased for each eye. In this design, changing diameter adds width to the haptic while maintaining chamber size. This helped address conjunctival compression in scleral lenses for children who usually have softer scleral rigidity.1 The patient tolerated the diagnostic trial well in office.
On dispense, the patient experienced immediate visual improvement to 20/25 OU, and her parents were trained in lens handling. At 2 weeks, mild rebound hyperemia after lens removal prompted ordering a second pair with a 17.0 mm diameter to increase haptic width and improve weight distribution. Symptoms resolved by the 1-month visit, and the prescription was finalized.
Six months later, the acuity decreased to 20/60 OD (OR = -1.00 yields 20/20) and 20/25 OS. Concerned about the myopic progression, the parents asked about additional interventions. The right eye distance power was updated, and a +2.50 ADD center distance bifocal was prescribed.
After several weeks of adaptation, the patient achieved 20/20 vision. After 3 years of biannual follow-up, the patient has shown no myopic progression and continues to wear her multifocal scleral lenses.
Discussion
This case demonstrates the value of a multifaceted approach to high astigmatism and early onset myopia. Incorporating center-distance multifocal supported myopia management alongside atropine,2,3 the patient achieved refractive and axial stability by age 9.
Conclusion
Scleral lenses, often reserved for corneal irregularities, can be an effective solution for young patients with high refractive error or astigmatism when traditional methods are inadequate. Combined with pharmacologic myopia control, scleral lenses can offer functional and long-term protective benefits.
References
- Francois, J. The importance of scleral rigidity in ocular tonometry. Indian J Ophthalmol. 1960;8(1):16-24.
- Walline JJ,Lindsley KB, Vedula SS, et al. Interventions to slow progression of myopia in children." Cochcrane Database Syst Rev. 2020;97(6):405-420.
- Gregory HR, et al. Visual performance of center distance multifocal contact lens fit using a myopia control paradigm. Optom Vis Sci 2021. March 1;98(3):272-279

To hear Dr. Shibayama discuss this case, click here.